
Mechanism of Dysfunction
The main predisposing factor for the development of bunionette is the impaired foot mechanics caused by a compromised of the arches (see Flat foot page for detailed information) particularly the lateral arch, therefore allowing the weight bearing stress to migrate further down and to the side of the foot altering pedal action forces resulting in a dropped 5th metatarsal head leading to an increase angulation at the level of the 5th metatarsal phalangeal joint.
Is important to point out that the main misalignment is not at the level of the deformity 5th metatarsal phalangeal joint (little toe), is at the joint prior, at the 5th metatarsal head.
Assessment Protocol
The entire lower extremity biomechanical chain must be evaluated as part of the foot/bunionette analyses as per the neurological and mechanical influences of the spine, hip, and knee.
Clinical assessment of the state of the all three arches and identify the key joint dysfunctions of the Ankle/Foot following by three set of X-ray analysis.
Anterior – Posterior (AP) X-ray ankle view is essential for proper diagnosing the master joint of the ankle (Tibia-Talus) as the origin of poor arch mechanics starts from a dysfunctional ankle joint leading to hypermobility compensations that causes the appearance of the bunionette.
Lateral Foot Xray view is important to check the degree of the total arch compromised, specially the lateral arch as per the direct influence it has with this deformity.
AP Xray foot view, aids to complete the total analysis of the transverse and lateral arches and is crucial to analyse the degree of the main bunionette misaligned joint (5th metatarsal head).
Treatment protocol
Due to the influences the foot arches have in the development of bunionette, arch rehabilitation must be incorporated as part of the overall treatment.
Foot Arch treatment: Specific adjustments of key bones of the ankle and foot (Talus, Navicular, Calcaneus and Cuboid) followed by a rehabilitation regime to strengthen the entire soft tissue arch support of the foot. In addition, application of tape and corrective orthotics may be needed as part of the early rehab program.
There are four direct important misalignments that needs to be addressed to aid on the reversion this deformity.
1 – Fifth metatarsophalangeal joint (little toe) capsule bulge reduction
2 – Adjustment of the main bunionette misaligned joint (5th metatarsal head)
3 – Adjustment of the fifth metatarsophalangeal joint
4 – Adjustment inferior of the 5th metatarsal head
Depending on the level of arch compromised and chronicity of the bunionette a minimum of 6 weeks up to 12 weeks of treatment care may be necessary to resolve this deformity.
Related Conditions
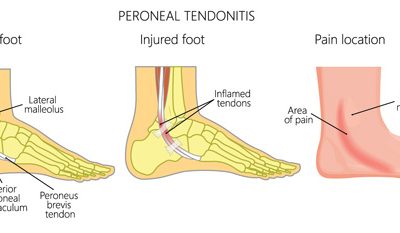
Peroneal tendinitis
Mechanism of...

Tibialis anterior tendinitis
Tibialis...

Ankle and foot fractures
Mechanism...